Following early-stage rehabilitation milestones; when swelling has settled, range of motion is restored, and gaitpatterns normalize, the mid-to-late phase of ACL rehabilitation becomes the determinant of long-term outcome. The progression from early-stage tomid-to-late phases, guided by objective criteria rather than fixed timelines, determines whether recovery is sustainable or whether subtle deficits predispose to reinjury.¹ The timing of transition varies among individuals;some athletes progress to mid-to-late phase work within 8-12 weeks, whileothers require additional time to satisfy early-stage criteria. This transitionrequires a shift in focus from protection and restoration toward progressiveloading and physical development.
Progression Benchmarks: The Critical Middle Phase
Early-stage rehabilitation milestones, whenachieved, provide the foundation for the mid-to-late phase: swelling ismanaged, range of motion is restored, and gait patterns are normalised. Thetiming of achievement varies among individuals based on operation type,post-operative response, compliance, and individual physiological recovery.However, subjective readiness frequently diverges from objective andphysiological readiness, regardless of post-operative week. This periodencompasses graft ligamentisation - where the graft tissue gradually remodelsto become a true ligament. This represents a phase of relative graftvulnerability, where progression requires careful planning.
The mid-to-late phase is where substantialneuromuscular and structural reconditioning occurs. This phase requires afundamental shift from protection and restoration toward progressive loadingand physical development. Strength development during this phase shouldprioritize absolute normalized capacity (body weight-normalized values) whilemonitoring limb symmetry (LSI). Research demonstrates that athletes whoprogress based on objective criteria, particularly absolute strength thresholdsrather than arbitrary timelines, show substantially lower reinjury rates - asmuch as 2-3 times lower than those who progress prematurely.1
Regarding time, research demonstrates thatreinjury risk progressively decreases with extended rehabilitation beyond 9months post-operatively, with each additional month providing continued riskreduction, particularly when combined with a criteria based return to sport.²This finding underscores that the 12-month rehabilitation window represents notan arbitrary timeline but a period sufficient for systematic adaptation acrossmultiple physical qualities and reinjury risk mitigation.
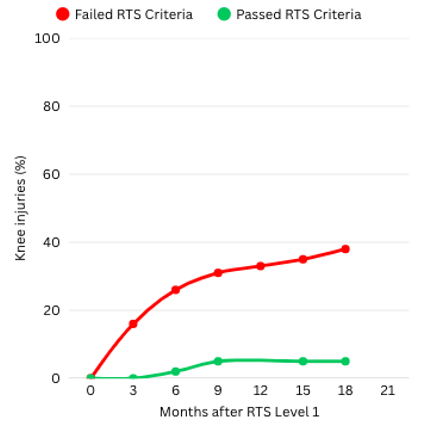
Figure 1. Knee reinjuries after return tolevel I sports in those who failed and those who passed return to sport (RTS)criteria prior to return.
Building capacity: Pillars of Rehabilitation
Strength development encompasses multiplesystems working synergistically. After ACL reconstruction, systematicrestoration across the kinetic chain is central to rehabilitation. This processinvolves key elements: absolute strength capacity, rate of force development(speed of force generation), power production, and the integrated developmentof energy systems (aerobic and anaerobic capacity) that support sustainedphysical effort and recovery.
1. Strength Development
The quadriceps demonstrate the slowestrecovery trajectory post-ACL reconstruction. Post-operative quadriceps strengthremains substantially reduced during the early phase, requiring systematicrestoration of absolute capacity, rate of force development, and powergeneration across the rehabilitation timeline.
Strength measurement using force plates ordynamometry provides objective assessment free from bias. Limb Symmetry Index(LSI) alone is insufficient as a marker, as both limbs may demonstrate symmetrywhile remaining underpowered relative to sport demands. Normalized strengthvalues (accounting for body weight) represent a more robust determinant ofcapacity. Early quadriceps strength gains during the first 12 weekspost-operatively demonstrate significant predictive value for strength recoveryat return-to-sport testing. Research demonstrates that quadriceps strength at12 weeks post-op explains 47% of the variance in quadriceps strength at thetime of return-to-sport testing, underscoring that early strength developmentstrongly influences late-stage strength outcomes.2 This findingreinforces the necessity of prioritizing quadriceps restoration during theinitial post-operative phase.
As strength develops, subsequent focusintegrates the rate of force development - the speed at which force can begenerated, which becomes increasingly important for dynamic sport tasks.
2. Unilateral Strength & Power Development
The focus of exercise shifts from bilateral tounilateral work. However, the former should not be eliminated, as it stillserves as an effective means of developing strength and power. Unilateralstrength encompasses proprioceptive integration, motor control, and thecapacity to generate and control force on a single limb. However, strengthalone is insufficient; rate of force development (RFD) - the speed at whichforce is generated, represents a critical component of readiness.
Sport movements occur at high velocities:cutting, deceleration, and rapid weight transfer happen in milliseconds,generating substantial force demands at the knee. Injuries in sport typicallyoccur during these high-speed, high-force events, and the injury mechanismunfolds within fractions of a second. An athlete with adequate strength butinadequate RFD cannot mobilize that strength quickly enough to stabilize theknee during rapid directional changes or unexpected perturbations. Theneuromuscular system must be trained to generate adequate force within the timewindow that sport demands impose. Without systematic development of RFD,athletes may possess strength in controlled testing environments but lack theability to stabilize during the uncontrolled, reactive demands of sport.Ultimately, the goal is for both bi and unilateral capacity for sport-specificdemands, and the ability to generate substantial force quickly when it mattersmost.
3. Load Progression & Building the Engine
Data-driven progression requires systematicmeasurement of exertion and intelligent load scaling. Rate of PerceivedExertion (RPE), velocity-based training metrics, and movement qualityassessment serve as guides for load progression.
Capacity encompasses absolute strength, forcegeneration speed, power output, and energy system development. Energy systemcapacity, the ability to sustain effort across varying intensities anddurations, is a distinct component of return-to-sport readiness. Aerobiccapacity supports recovery between high-intensity efforts and trainingtolerance. Anaerobic capacity underpins sport-specific demands: acceleration,change-of-direction, and repeated sprinting efforts. Progressive training mustaddress both energy systems. For example, early phases may emphasize aerobicbase development and sustained efforts; intermediate phases layer in repeatedhigh-intensity efforts with structured recovery intervals; late phases demandsport-specific intensity matching competition demands. Keep in mind that thesecan and should occur concurrently, however, the focus at a particular timepointmay lean more towards one particular system than the other.
The goal is to systematically increasephysical capacity across multiple domains - the ability to tolerate load,generate force, sustain effort, and recover appropriately betweenhigh-intensity efforts. If movement quality diminishes under fatigue, it isimportant to make the distinction between lack of strength and/or endurance,or, energy system capacity.
RestoringMovement & Confidence
Rehabilitation progression from early-phasemovements toward sport-specific demands follows a graded hierarchy. Subsequentphases introduce proprioceptive demand, single-leg loading, directionalvariation, and multi-planar movement patterns. Late-phase progressionemphasizes sport-specific movements including cutting drills, decelerationcontrol, and reactive directional changes performed at training intensities.Throughout this progression, movement quality must remain high. Video analysis,force plate data, and movement assessment ensure optimal control andconfidence. Should compensatory patterns emerge during movement tasks, or, datais skewed away from what is expected, then it is vital to determine why; is itlack of strength, control, exposure. It is important that refining thesemovement patterns precedes further progression.3
In addition, the same rigor must be applied tomovement quality outside of strength training. Inadequate movement quality inrunning, deceleration or directional changes may be subtle signs that theathlete is either lacking confidence, or, the strength to load the knee. Thiscould also force the contralateral limb to absorb forces that the surgical kneecannot tolerate, substantially elevating contralateral injury risk. Systematicattention to movement integrity, running mechanics, controlled deceleration,and appropriate weight transfer through direction changes is thereforeessential for mitigating re-injury.

Figure2. Example of SMAS (Sprint Mechanics Assessment Score).
BeyondIsolated Training: The Case for Comprehensive Capacity
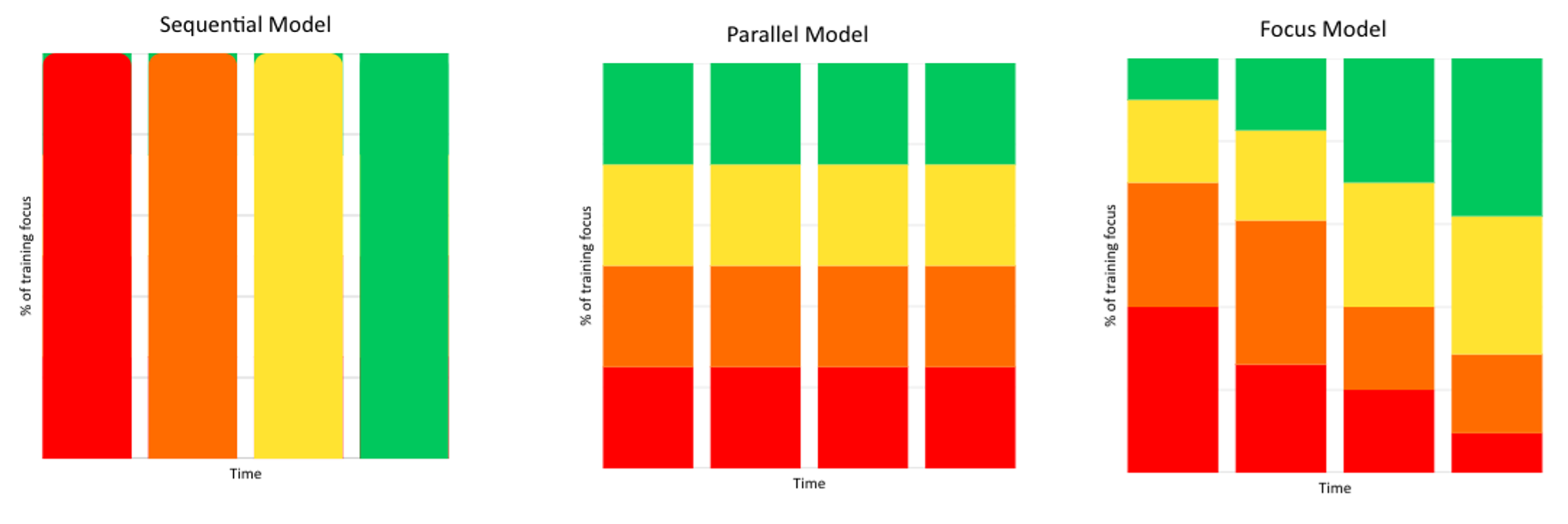
A critical distinction exists betweenstructured blocks of training (e.g., focusing on strength development, thentransitioning to power, then movement complexity) and the fundamentally flawedapproach of isolating individual physical qualities for extended periods.Isolated, compartmentalized training approaches that emphasize a singlephysical quality for weeks or months do not allow for sufficient time toproduce sustained neuromuscular adaptation across the spectrum of demandsrequired for sport performance.
Rather, comprehensive periodized programmingmaintains concurrent development of multiple physical qualities: strength,power, proprioception, movement control, and psychological readiness,throughout all phases of rehabilitation. Within this framework, blocksemphasizing particular qualities create structure without sacrificing fluidity.Athletes continuously expose themselves to varied demands, allowing theneuromuscular system sufficient time to adapt to each quality. This integratedapproach allows for progressive exposure to complexity and intensity. Therepeated, gradual exposure across time, not isolated focus, drives sustainableadaptation.
Common Rehabilitation Challenges
Persistent Strength Deficits
Absolute normalised strength deficits, whereathletes fail to reach adequate strength per kilogram of body weight, signalincomplete motor recruitment or neuromuscular adaptation. Performance deficitsfrequently persist well into the mid-to-late rehabilitation phase and beyond.Research demonstrates that jump performance deficits persist even at 9 monthspost-operatively despite standard rehabilitation protocols, underscoring thatdeficits do not spontaneously resolve and require targeted intervention ratherthan expectation of passive adaptation.4 LSI may appear adequatewhile absolute strength remains compromised; addressing absolute strengthdeficiencies takes priority.
Final Word
ACL reconstruction requires a systematic12-month rehabilitation progression to adequately rebuild strength, movementquality, and neuromuscular confidence. The distinction between athletes whoachieve sustainable return-to-sport and those who experience reinjury mayreflect adherence to criterion-based progression versus timeline-basedprogression. Objective measures, including strength symmetry, hop testperformance, movement quality, serve as gates between rehabilitation phases andinform return-to-sport decision-making.5 In addition, sufficienttime to build the physical qualities necessary to return to sport cannot beoverstated.
References
- Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med. 2016;50(15):942-947. doi:10.1136/bjsports-2016-096031
- Hannon JP, Wang-Price S, Goto S, Singleton S, Dietrich L, Bothwell J, Bush C, Garrison C. Twelve-week quadriceps strength as a predictor of quadriceps strength at time of return to sport testing following bone-patellar tendon-bone autograft anterior cruciate ligament reconstruction. Int J Sports Phys Ther. 2021;16(3):681-688. doi:10.26603/001c.23421
- Hewett TE, Paterno MV, Myer GD. Strategies for enhancing proprioception and neuromuscular control of the knee. Clin Orthop Relat Res. 2012;402:76-94. doi:10.1097/00003086-200209000-00008
- Costley JAE, Miles JJ, King E, Daniels KAJ. Vertical jump impulse deficits persist from six to nine months after ACL reconstruction. Sports Biomech. 2023;22(1):123-141. doi:10.1080/14763141.2021.1945137
- Lynch AD, Logerstedt DS, Grindem H, et al. Consensus criteria for defining "successful outcome" after ACL reconstruction: a Delaware-Oslo ACL cohort investigation. Br J Sports Med. 2015;49(5):335-342. doi:10.1136/bjsports-2013-093437