The most complex joint in our body, the knee allows us to walk and run while supporting the weight of our entire body, making them an essential component of our daily activities. Our knees experience routine changes as we age, which can lead to a condition known as osteoarthritis.
The most prevalent joint disease, osteoarthritis, affects 528 million people globally, with 3.6 million of those cases occurring in Australia alone. The weakening of articular cartilage resulting in knee osteoarthritis causes pain, stiffness, and oedema that gets worse with movement.
Anatomy of the Knee Joint
Before we dive into the details of Osteoarthritis, it is essential to understand how knee works. The knee is a complex hinge joint which comprises of three bones: Femur, Tibia and Patella. These bones are connected by Ligaments that stabilise the joint, namely the Anterior, Posterior, Medial and Lateral Cruciate Ligaments. The meniscus acts as a shock absorber for movement and loading, particularly important for the medial meniscus as more than 70% of your bodyweight is absorbed through the tibia on the medial side.
In the knee joint, two bony connections are formed by three bones. The strongest joint, supporting nearly the whole weight of the body, is that between the femur and the tibia. The one between the patella and femur, on the other hand, provides a seamless channel for the forces generated by the contraction of the quadriceps.
Friction at the bony unions is prevented by the presence of cartilages which act as shock absorbers, allowing pain-free motion. Cartilage lays over bone and acts to minimise joint friction. It is the degeneration of these cartilages which causes Osteoarthritis.
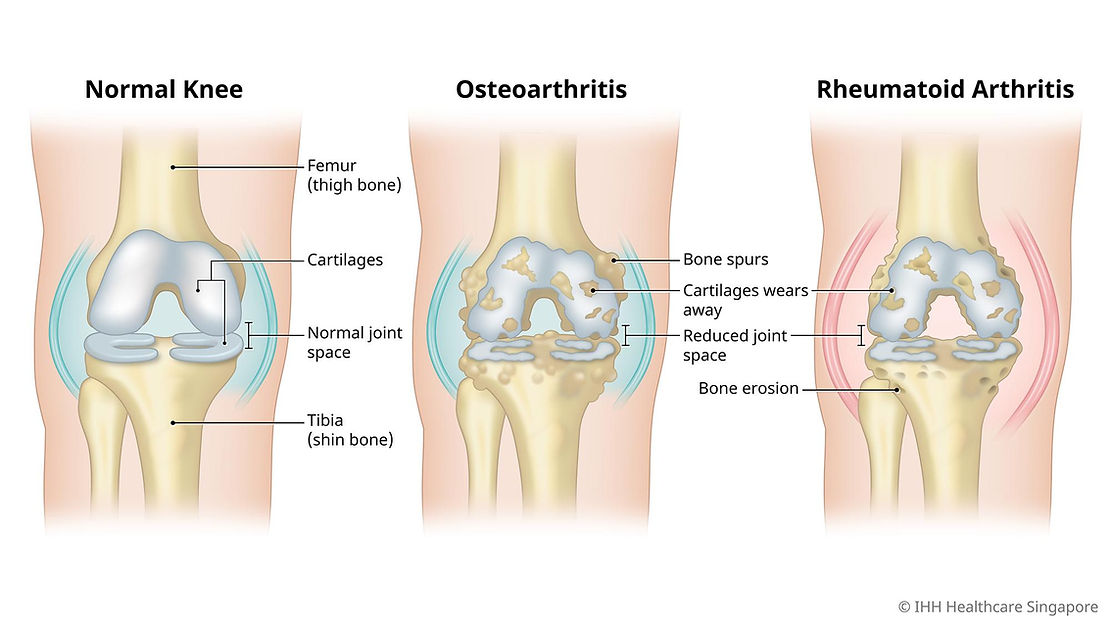
Osteoarthritis vs Rheumatoid Arthritis
While both Osteoarthritis and Rheumatoid Arthritis affect joints, they differ vastly in their aetiology and characteristics.
Osteoarthritis is the most prevalent joint disease in people aged over 45, mostly females. It is classified into two types:
- Primary: unknown cause, usually attributed to normal wear and tear of cartilages
- Secondary: known cause, e.g. Obesity or Joint hypermobility.
Osteoarthritis results in knee pain and disability which can significantly impact a person's quality of life, making it difficult to perform daily activities such as walking and climbing stairs.
On the other hand, Rheumatoid Arthritis is an autoimmune condition; in which the body mistakenly attacks its own tissues; in this case the joint lining (synovial membrane), resulting in pain and immobility. While rheumatoid arthritis has a far more extensive treatment regimen focused on the underlying inflammatory illness, knee osteoarthritis mostly focuses on managing cartilage deterioration and improving joint function. Anti-rheumatic medications has significantly improved the severity and improved quality of life of rheumatoid arthritis patients.
Diagnosing Knee Osteoarthritis and Rheumatoid Arthritis
To identify osteoarthritis as soon as possible, several steps are followed. The standard diagnostic process typically consists of the following steps: medical history, clinical evaluation, and imaging investigations such as MRIs and X-rays to confirm the diagnosis.
- Medical History: the medical professional will start by taking a history of osteoarthritis in your family, injuries, age, sex and lifestyle factors, any of which may contribute to the development of this disease.
- Clinical Assessment: The healthcare professional will look for clinical signs of swelling, and limited range of motion along with a comprehensive strength and function assessment. They may also inquire for pain patterns, and relieving or exacerbating factors.
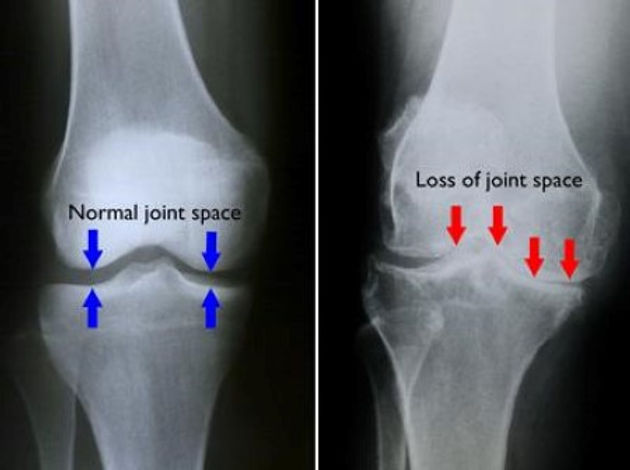
- Imaging: The first line of imaging evaluation is an X-ray. It is used to search for indicators of osteoarthritis, such as cysts and sclerosis in the subchondral region, creation of bony spurs, and narrowing of the knee joint space. magnetic resonance imaging (MRI) may be useful if other sources of knee pain are suspected.
Rehabilitation & Therapy
Management of Osteoarthritis is divided into conservative and surgical options. The first and foremost step is educating the patient about the condition and then employing the management steps:
- Physiotherapy: Physiotherapy plays a major role in the management and improvement of Osteoarthritis patients. A comprehensive assessment of your strength, function, range of motion and balance provides a detailed baseline and allows for data-driven rehab planning. Development of a custom exercise plan that includes supervised and at-home training is the first step taken by a Physiotherapist. Exercises are focused on strengthening the muscles surrounding the knee which improves joint mobility, and flexibility enhancing the quality of life. Range of exercises which include motion exercises, weight training and low-impact activities like swimming contribute to pain alleviation if continued regularly.
- Weight Control: Being overweight (Body Mass Index greater than 25) means excessive pressure on the knee joint, flaring up symptoms of osteoarthritis, hence it is important that weight should be managed to reduce overload.
- Assistive Devices: The knee joint can be supported externally to provide stability by the use of orthotic devices such as knee braces, knee taping as well as specialised footwear. Knee taping has been found effective in unloading the soft tissues and aligning the patella, reducing the pain in the process. Specialised footwear and accessories like lateral show wedges have been found in studies, to be effective in reducing knee loading, and alleviating pain and symptoms associated with Osteoarthritis.
- Medications: If the pain and disability are not managed with physiotherapy alone, then medical options like NSAIDs may be prescribed by your GP to manage the pain and inflammation. In severe cases, steroids and hyaluronic acid are directly injected into the joint space for direct action.
Injury Prevention
It is well-known that prevention is better than a cure. Preventing and minimising the development of osteoarthritis includes:
- Regular Exercise: Engaging in low-impact exercises like stationary cycling, and swimming initially can help to reduce knee joint loads whilst ensuring strength and function adaptations are still made.
- Practice Joint Friendly Activities: Adjust exercises that put undue stress on the knees. For example, use appropriate body mechanics when carrying heavy objects to prevent excessive joint stress.
- Muscle Strengthening: Weight training to strengthen the muscles surrounding the knees, including hip muscles plays an essential role in preventing recurrent injury to the knee joint.
- Put on the Right Shoes: Select footwear that provides adequate arch support and cushioning to lessen the strain on the knees whilst completing daily tasks.
- Maintain a Healthy Weight: Maintaining a healthy lifestyle that includes regular exercise and a balanced diet will help control body weight and lessen the strain on the knee joints.
To Finish
Knee osteoarthritis is a prevalent disease that has to be effectively managed using a comprehensive strategy. Crucial actions include being aware of the symptoms and obtaining a diagnosis as soon as possible. The cornerstone of treatment is rehabilitation and therapy, which includes physical therapy, weight control, and assistive equipment. In addition, injury prevention techniques enable people to protect their knees and maintain long-term joint health.
Remember that controlling knee osteoarthritis can be greatly impacted by early intervention and proactive lifestyle choices. Early screening of your joint health can ensure a personalised program is implemented to reduce the risk of developing knee osteoarthritis.
If you are experiencing knee pain or are looking to obtain comprehensive testing and screenign to enhance your knee function and minimise the risk of developing knee arthritis? Book in for a physiotherapy or testing & screening consultation for individualised, tailored guidance or join our Strong Knees program! Your journey to strong knees for the future starts here 💫 💪
Book Now
References
Abulhasan, J. F., & Grey, M. J. (2017). Anatomy and Physiology of Knee Stability. Journal of Functional Morphology and Kinesiology, 2(4), 34. https://doi.org/10.3390/jfmk2040034
Radu, A., & Bungau, S. G. (2021). Management of Rheumatoid Arthritis: An Overview. Cells, 10(11), 2857. https://doi.org/10.3390/cells10112857
Hsu H, Siwiec RM. Knee Osteoarthritis. In: StatPearls. StatPearls Publishing, Treasure Island (FL); 2022. PMID: 29939661
Collins NJ, Hart HF, Mills KA. Osteoarthritis year in review 2018: rehabilitation and outcomes. Osteoarthritis and cartilage. 2019 Mar 1;27(3):378-91
Conaghan PG, Dickson J, Grant RL (2008) Care and management of osteoarthritis in adults: summary of NICE guidance. BMJ 336, 502–3
Disclaimer: This blog is for informational purposes and should not be considered a substitute for professional medical advice. Please consult with our qualified healthcare providers for personalised recommendations related to your specific condition and needs.