The knee is one of the most intricate structures supporting the body's weight, making it susceptible to injuries. Meniscus tears primarily targets physically active people i.e. athletes, runners and laborer's, with an incidence of 8.7 per 1000 people. Usually a result of a knee twist or torsion, it affects 13% of the general population.
If you or someone you know has recently experienced knee pain, then stick to the endo fo this article to understand the anatomy of the meniscus, physiology, symptoms, diagnosis and rehabilitation
Anatomy of the Knee
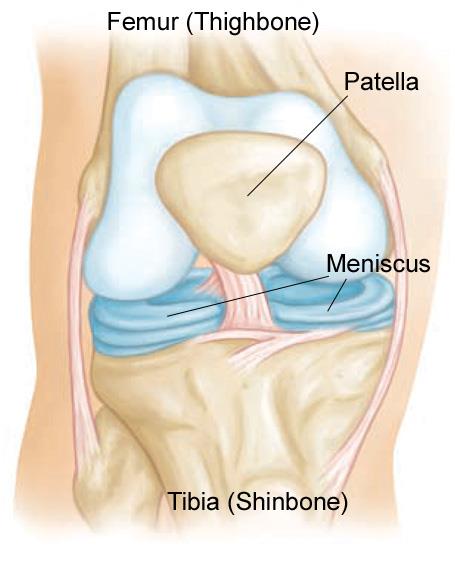
Before we dive into the details of Meniscal tears, it is essential to understand how the knee works. It compromises of three bones: Femur, Tibia and Patella which are connected by Ligaments that stabilise the joint; namely Anterior Cruciate, Posterior Cruciate, Medial and Lateral Collateral Ligaments.
The strongest joint, supporting nearly the whole weight of the body, is that between the femur and the tibia, or the tibiofemoral joint. The patellofemoral joint (between the patella and femur) on the other hand, provides a seamless channel for the forces generated by the contraction of the quadriceps.
The meniscus sit between the femur and the tibia. These C shaped cartilages that act as shock absorbers and distribute weight throughout the knee joint. There are two meniscus present, one on each side namely the Lateral and Medial Meniscus. Medial Meniscus has more attachments to the knee joint which makes it fixed in its position hence more prone to injury.
Physiology of Meniscus Tears
- Shock Absorbers: A jump from a significant height incurs significant forces through the knee, with the meniscus providing shock absorption during jumps, running and daily function. They absorb and distribute forces applied to the knee, protecting the underlying articular cartilage from stress. Unnatural forces such as excessive twisting and torsion can lead to a meniscus tear.
- Joint Stability: The meniscus improve joint stability through its crescent shape anatomy, minimising shear forces. Thus any excessive shear force can lead to a meniscal tear.
- Weight Distribution: As mentioned previously, the knee joint bears the weight of the body and the meniscus play a key role in weight and force distribution during loading.
Classification
Meniscus tears are classified by:
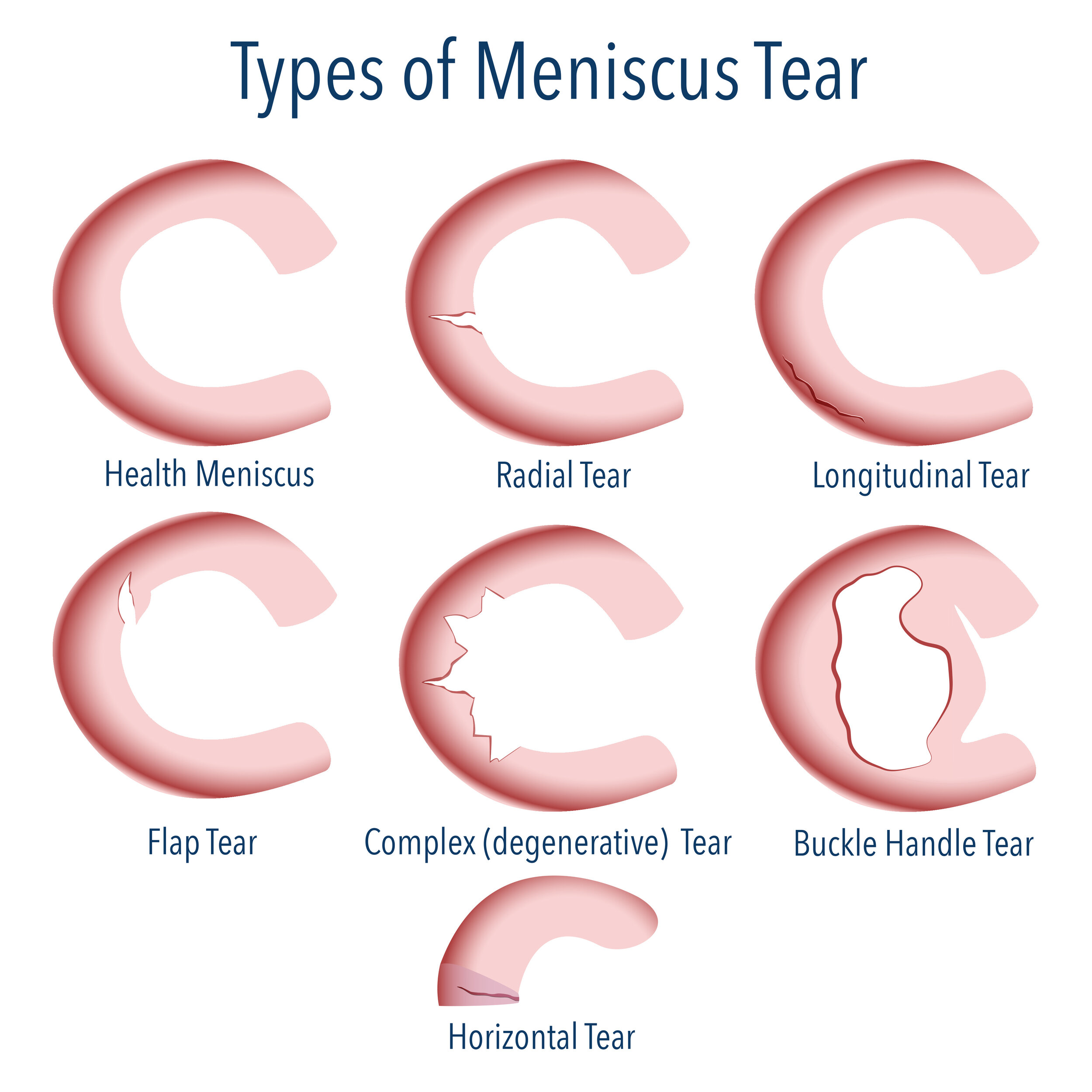
- Location: The meniscus is divided into two portions according to location. The lateral meniscus has less force distributed through it (approximately 30%) whilst the medial meniscus bears up to 70% of body weight force, making it more susceptible to injury. Various types of tears exist including: radial, longitudinal, flap, complex, horizontal and bucket handle.
- Onset:Acute Injury: These meniscal tears are primarily traumatic due to sudden excessive twisting or torsional motion of the knee which leads to a tear in the meniscus Degenerative Injury: Through chronic changes and repetitive actions, chronic tears can occur within the meniscus.
Signs & Symptoms
Meniscus tears can present with a wide array of symptoms:
- Pain: Pain can range in intensity and location i.e. Pain on the outer side of the knee may indicate a lateral meniscus tear and pain on the inner side may indicate a more common medial Meniscus tear. Clinicians further test this sign by eliciting pain in positions like Squatting or Twisting to confirm the diagnosis of a Meniscus tear.
- Swelling: Acute injury to the knee resulting in a Meniscus tear can cause an inflammatory process, resulting in swelling and oedema. The swelling phase may reach its peak in 2 to 3 days.
- Stiffness: Pain in the knee and inflammation can lead to restricted joint range of motion and stiffness.
- Locking, Clicking & Giving Way: A meniscal tear may inhibit normal joint movement and result in locking, clicking or the knee giving way during certain ranges of motion/actions.
Rehabilitation of Meniscus Tears
Every patient is different due to the type, severity and location of injury. Dependent on the type of injury, a surgical opinion may be required to repair the torn meniscus. Conservative rehabilitation includes acute management which includes the following:
- Rest: by reducing activities and providing support to tissues. This may include the use of crutches to offload the injured knee.
- Ice: Applying ice to the affected area several times daily for 20 minutes each reduces joint swelling and pain.
- Compression: Serves to reduce swelling and improve joint motion.
After this initial phase, conservative management starts with regaining normal joint range of motion and basic strength qualities. Isolated strengthening of the quadriceps and hamstrings is progressed to more functional loading exercises with the goal to return to pre-injury functional levels. During the rehabilitation process, joint stability, proprioception and balance exercises are also implemented to enhance joint health and reduce the risk of re-injury.
In some severe cases where the patient does not respond to conservative therapy or the tear is large or unstable, surgery may be considered as the treatment mode. Various procedures such as Meniscus Repair using sutures and Arthroscopic Meniscectomy to repair the Meniscus. When repair is not possible then Surgeons will remove a portion of the Meniscus.
Injury Prevention - Stability, Hip Control & Specificity of Training
Preventing Meniscus tear is always better than treating it. Here are some tips to prevent a tear completely or if already occurred, prevent its recurrence:
- Improve knee strength - specifically quadriceps, adductors and hamstring strength
- Optimise kinetic chain strength and stability - this includes strengthening the lateral and posterior hip muscles to enhance proximal chain stability
- Function-sport-specific training that includes tasks that you regularly perform to improve stability (jumps, landings, steps, pivots)
To Finish
Although meniscus tears a common knee joint injury, it is a treatable condition with positive outcomes for both conservative and surgical rehabilitation management. Early diagnosis is important to establish the most appropriate route of management. Acute phase management, along with a progressive, periodised rehabilitation program that targets the deficits present improves outcomes and return to function. Optimising knee stability, strength along with hip function and control help to reduce the risk of injury and enhances function.
If you are experiencing knee pain or symptoms, consider a physiotherapy consultation or the Strong Knees Program for tailored, data-driven guidance and therapy.
Book Now
References
Donohue MA, Zhou L, Haley CA. Meniscus Injuries in the Military Athlete. J Knee Surg. 2019 Feb;32(2):123-126
Abulhasan, J. F., & Grey, M. J. (2017). Anatomy and Physiology of Knee Stability. Journal of Functional Morphology and Kinesiology, 2(4), 34
Fox, J. S., Wanivenhaus, F., Burge, A. J., Warren, R. F., & Rodeo, S. A. (2015). The human meniscus: A review of anatomy, function, injury, and advances in treatment. Clinical Anatomy, 28(2), 269-287.
Fox AJ, Bedi A, Rodeo SA. The basic science of human knee menisci: structure, composition, and function. Sports Health. 2012 Jul;4(4):340-51
Chen HN, Yang K, Dong QR, Wang Y. Assessment of tibial rotation and meniscal movement using kinematic magnetic resonance imaging. J Orthop Surg Res. 2014 Aug 21;9:65
Gupte, C., & Mart, P. S. (2013). The acute swollen knee: Diagnosis and management. Journal of the Royal Society of Medicine, 106(7), 259-268.
Disclaimer: This blog is for informational purposes and should not be considered a substitute for professional medical advice. Please consult with our qualified healthcare providers for personalised recommendations related to your specific condition and needs.