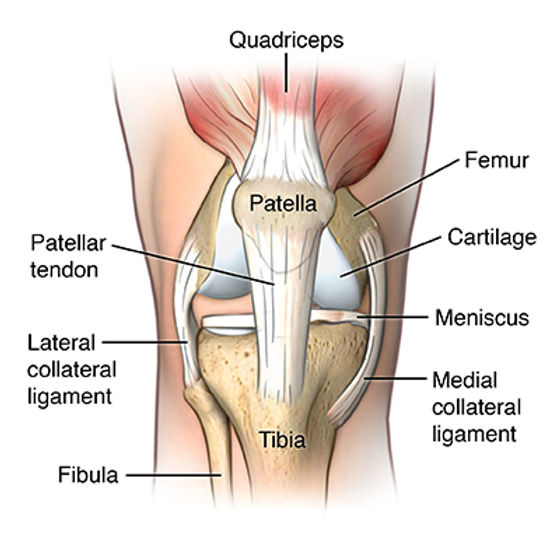
As one of the most common overload sports injuries, Jumpers Knee affects the the strong band of tissue that attaches the kneecap (patella) to the shinbone (tibia) - the patellar tendon. As the name suggests, athletes who participate in sports that involve repetitive jumping and landing such as basketball, volleyball, football, CrossFit and running are at a higher risk of developing Jumper’s knee.
The prevalence of Jumper's knee (or patella tendinopathy) is high, with evidence suggesting that approximately 45% of all professional athletes and 14% of recreational athletes have experienced Jumper’s knee symptoms at some time. That said, each sport has different risk profiles for developing Jumpers knee, with volleyball players at the highest risk (14.4%) whereas football players were relatively reduced at 2.5% incidence reflecting the demands of the sport on the patella tendon.
If you have recently experienced knee pain or suspect you may have Jumpers knee, then stick till the end of this article to find out what this condition is, how it develops and how we can effectively manage it.
What is Jumpers Knee? What are the Key Risk Factors?
As the name suggests, athletes involved in sports that require frequent jumping and landing i.e Volleyball, Basketball, CrossFit, are susceptible to developing Jumpers knee. The continuum model from Jill Cook’s research suggests that Tendinopathy develops in three phases: reactive tendinopathy, tendon dysrepair and then degenerative tendinopathy. This means that a susceptible tendon may not be able to withstand normal loading forces leading to reactive tendinopathy. It is not well known at which age tendons become susceptible to tendinopathy, as tendon’s structure matures during puberty indicating that Jumper's knee can happen at any age. This theory is supported by the fact that Jumper's knee has also been diagnosed in people as young as 16. Frequent overloading of the tendon usually from jumping and landing results in the onset of pain which can be debilitating and career-ending for professional athletes.
Research has suggested additional risk factors that predispose an athlete to injury, as follows:
- Overuse: Ignoring an underlying problem of knee pain, with a continued training pattern can change tendon pathology and lead to tendinopathy. Hence those who suspect they are suffering from Jumpers knee should seek assessment to reduce the risk of chronic patella tendinopathy
- Biomechanics: Proper technique is pivotal for performance as well as injury prevention. Poor landing technique, along with proximal hip and groin mechanics can increase loading through the anterior chain, increasing tendon load and leading to tendinopathy
- Gender: Gender has a role to play in Tendinopathy with men appearing to be at an increased risk for developing Jumpers knee.
- Hamstring Extensibility: Poor hamstring mobility and extensibility can increase quadriceps loading, consequently increasing patella tendon loading during function
Signs & Symptoms to Look Out For
Early recognition of symptoms plays a pivotal role in prompt diagnosis and appropriate treatment of Jumper’s knee. The following symptoms indicate the development of Patellar tendinopathy:
- Pain: A classic pain in the kneecap region which has a characteristic onset at the start of the activity might be indicative of Jumper’s knee. Pain responds variably to warm-up, some people may experience a flare-up while others feel relief from pain. A very indicative feature of Jumper’s knee is pain on prolonged sitting especially whilst driving. Pain can then affect daily function such as stair climbing, waling up/down hills and leaning on the effected knee.
- Stiffness: Hamstring and quadriceps may experience an increase in stiffness, leading to poor range of motion. Additionally, the patellofemoral joint may become stiff, reducing patella mobility. Stiffness of the knee and tendon is generally noted in the morning upon wakening, although this is not always present.
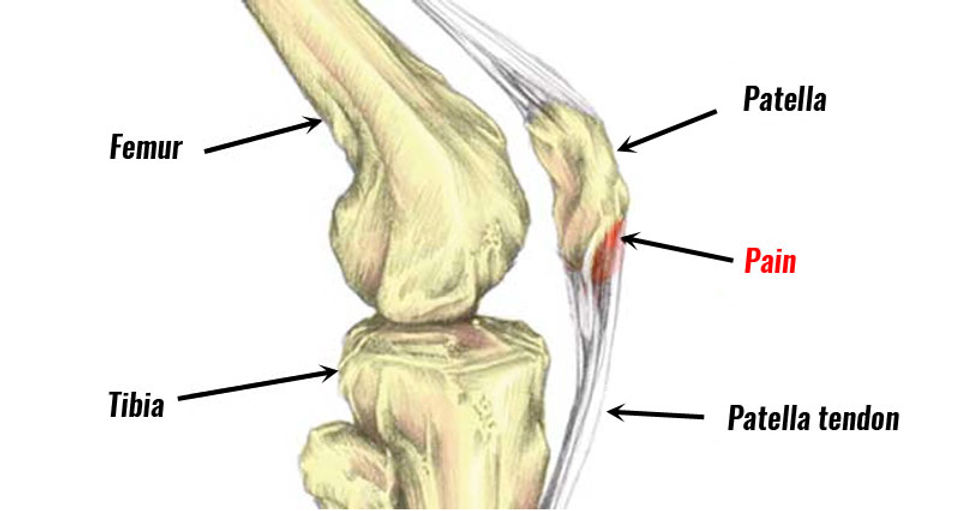
- Tenderness: Particular tenderness is noted at the inferior pole of the patella where the tendon attaches into the bone
Management of Jumpers Knee
Understanding the tendon’s function and the stage of pathology is crucial to effective management. For an acute tendonitis (inflammation of the tendon), rest and anti-inflammatories can reduce pain along with a graduated rehab program.
That said, long standing chronic tendinosis requires a well designed loading and rehabilitation plan to enhance tendon health and function. Rest unfortunately fails to improve chronic tendinopathies, instead resulting in deconditioning to the tendon and surrounding muscles.
The type of exercises employed and how these exercises are performed are important for chronic tendinopathies. The two types of muscle contractions that are important in tendinopathy rehabilitation are: isometric and eccentric exercises
- Isometric Loading: Isometric exercises involve only muscular contractions sparing joint movements. These exercises allow joint strengthening without putting an undue amount of strain on it, reducing pain.
- Eccentric Loading: Eccentric exercises focus on the lengthening phase of muscular contraction focusing on muscle adaptability and may be gradually added into the rehabilitation regimen. Eccentric exercises include single-leg decline squats and weighted bilateral squats.
Load Management - the Unsung Hero
As described, the primary mechanism of tendinopathy is caused by to overloading of the Patellar tendon. It is crucial to manage your training loads during rehabilitation to avoid spikes to loading and subsequent pain. The loading of the knee should be gradual and carefully monitored to avoid any undue stress on the Patellar tendon. Rest periods between heavy strength loading days are crucial, as this allows the tendon to adapt to the stress placed upon it and strengthen.
Optimising your warm-up and cool-down can assist in enhancing tendon extensibility and function for upcoming training, reducing pain onset and intensity. During latter phases of rehab, a maintenance plan is developed to ensure tendon adaptations continue and reduce injury risk.
To Finish
Although Jumpers knee affects a wide range of active individuals, it is a treatable condition with effective rehabilitation and management. Early management is crucial to reduce the risk of tendinitis developing into chronic tendinosis. Effective strength rehabilitation programming and load management are the key to Jumpers knee management. A holistic approach is also important - to identify the causative factors to developing Jumpers knee (biomechanics, loading, weakness) to ensure risk of re-injury is reduced and performance is optimised.
If you’re experiencing symptoms or have flair ups in knee pain, consider a physiotherapy consultation or musculoskeletal screening and testing consultation for tailored, data-driven guidance.
Book Now
References
Lian OB, Engebretsen L, Bahr R. Prevalence of jumper's knee among elite athletes from different sports: a cross-sectional study. Am J Sports Med. 2005 Apr;33(4):561-7
Zwerver J, Bredeweg SW, van den Akker-Scheek I. Prevalence of Jumper's knee among nonelite athletes from different sports: a cross-sectional survey. Am J Sports Med. 2011 Sep;39(9):1984-8. doi: 10.1177/0363546511413370. Epub 2011 Jul 7. PMID: 21737835.
Rudavsky A, Cook J. Physiotherapy management of patellar tendinopathy (jumper's knee). J Physiother. 2014 Sep;60(3):122-9. doi: 10.1016/j.jphys.2014.06.022. Epub 2014 Aug 3. PMID: 25092419.
J.E. Gaida, J.L. Cook, S.L. Bass, S. Austen, Z.S. Kiss Are unilateral and bilateral patellar tendinopathy distinguished by differences in anthropometry, body composition, or muscle strength in elite female basketball players? Br J Sports Med, 38 (2004), pp. 581-585
K. Gisslen, C. Gyulai, P. Nordstrom Alfredson H. Normal clinical and ultrasound findings indicate a low risk to sustain jumper's knee patellar tendinopathy: a longitudinal study on Swedish elite junior volleyball players. Br J Sports Med, 41 (2007), pp. 253-258
H. Visnes, R. Bahr Training volume and body composition as risk factors for developing jumper's knee among young elite volleyball players Scand J Med Sci Sports, 23 (2013), pp. 607-613
J.L. Cook, K.M. Khan, Z.S. Kiss, C.R. Purdam, L. Griffiths Prospective imaging study of asymptomatic patellar tendinopathy in elite junior basketball players J Ultrasound Med, 19 (2000), pp. 473-479
S. Edwards, J.R. Steele, D.E. McGhee, S. Beattie, C. Purdam, J.L. Cook Landing strategies of athletes with an asymptomatic patellar tendon abnormality Med Sci Sports Exerc, 42 (2010), pp. 2072-2080
A. Frohm, T. Saartok, K. Halvorsen, P. Renstrom Eccentric treatment for patellar tendinopathy: a prospective randomised short-term pilot study of two rehabilitation protocols Br J Sports Med, 41 (2007), p. e7
Khan KM, Bonar F, Desmond PM, Cook JL, Young DA, Visentini PJ, Fehrmann MW, Kiss ZS, O'Brien PA, Harcourt PR, Dowling RJ, O'Sullivan RM, Crichton KJ, Tress BM, Wark JD. Patellar tendinosis (jumper's knee): findings at histopathologic examination, US, and MR imaging. Victorian Institute of Sport Tendon Study Group. Radiology. 1996 Sep;200(3):821-7
Peers KH, Lysens RJ. Patellar tendinopathy in athletes: current diagnostic and therapeutic recommendations. Sports Med. 2005;35(1):71-87
Disclaimer: This blog is for informational purposes and should not be considered a substitute for professional medical advice. Please consult with our qualified healthcare providers for personalised recommendations related to your specific condition and needs.