Hip pain is a debilitating condition, hindering your daily activities and athletic performance? . It may be a symptom of several conditions such as structural issues, bursitis, labral tears or arthritis to name a few and where movement aggravates discomfort and pain.
One common pain diagnosed from a complaint of lateral hip pain is Greater Trochanteric Pain Syndrome (GTPS). This relatively common condition is typically characterized by pain over the trochanteric region and is often diagnosed in patients complaining of lower back, gluteal, hip and thigh pain. This often-debilitating ailment can impact general quality of life and athlete performance. If you or someone you know is experiencing symptoms of hip pain and discomfort, then please read on to understand anatomy of the hip region, an explanation of GTPS, symptoms, risk factors and treatment/management of the condition.
What is Greater Trochanteric Pain Syndrome?
Greater Trochanteric Pain syndrome (GTPS)is a relatively common condition, affecting gluteal tendons and bursa, when repetitive friction between the greater trochanter and iliotibial band induces trauma of the gluteal tendon at the greater trochanter insertion site. Research highlights an occurrence rate of 15% in females and 6.6% in males, indicating potential sex-related risk factors. The condition is characterised by pain over the lateral aspect of the thigh, exacerbated during high impact physical activity, climbing, sitting or lying down for prolonged periods.
Examination and testing to produce a clinical diagnosis include palpation of the great trochanter and the FABER test, (ie; Flexion Abduction and External Rotation), where the test induces a pain reaction.
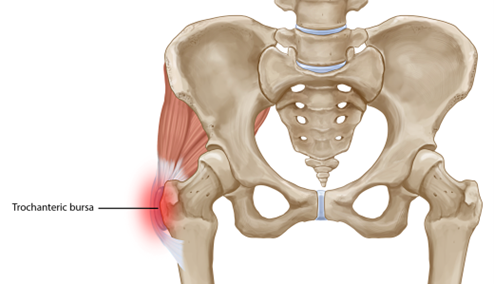
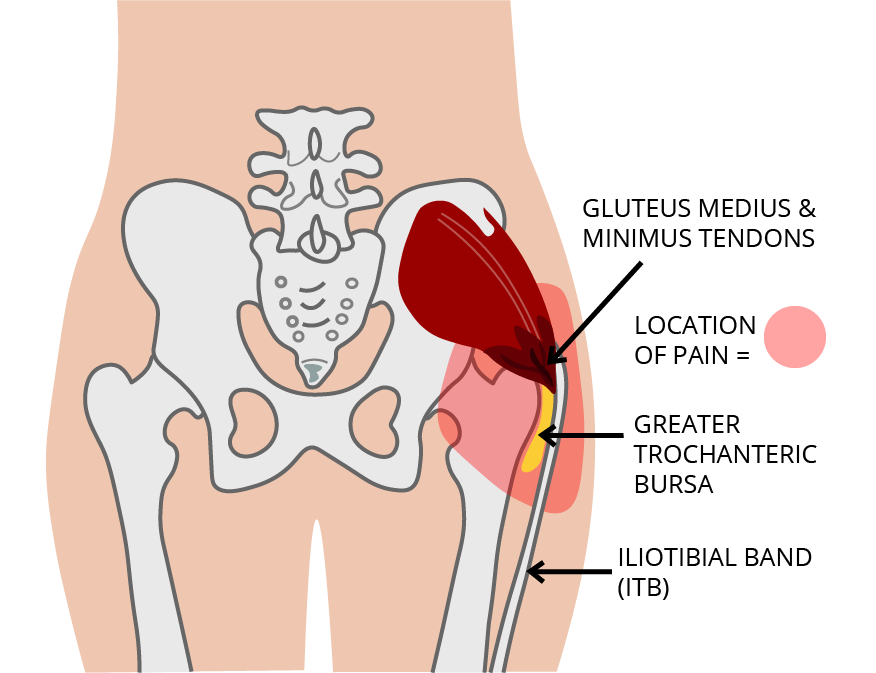
The Greater Trochanter is located on the top most portion of the femur bone, forming a bony bulge. Several muscles attach to the femur bone, namely the gluteus medius and tensor fasciae latae (TFL).The iliotibial band, a thick connective tissue band, also passes over the greater trochanter as it runs along the hip to the knee joint. The lateral hip anatomically constitutes of 6 bursa. Bursae are the spaces between anatomical structures with the primary aim of reducing friction to ensure smoothness and protection during movement. Bursa are implicated in Greater Trochanteric Pain Syndrome where GTPS may encompass trochanteric bursitis.
The Iliotibial band is of particular significance in patients diagnosed with GTPS when movement (running, walking, cycling) causes the ITB to articulate and friction against the greater trochanter's bony protrusion, causing discomfort, pain and inflammation, especially felt on the outside of the hip. Trochanteric bursitis diagnosis from a bruised Iliotibial band that irritates the bursa can also cause fluid accumulation and inflammation.
Important structures that articulate with the Greater Trochanter are the tendons of Gluteus Medius and Minimus. These tendons can become inflamed due to overuse, resulting in their thickening; a process known as tendinopathy. The research suggests injuries to these tendons are primarily involved (rather than trochanteric bursitis) in the development of Greater trochanter pain syndrome.
Signs & Symptoms of Greater Trochanteric Pain Syndrome
The term Greater Trochanteric Pain Syndrome suggests an amalgamation of a range of symptoms. The hallmark symptom is pain in the lateral hip region encompassing the greater trochanter region.
Pain is subjective and can range from light to sharp pain progressing to the chronic stage as an uneasy dull ache. This pain is very commonly associated with lower back pain. Daily life activities such as running, climbing stairs, and sleeping on the affected site may also worsen the pain. [3]
Additional typical GTPS symptoms and indicators include:
- Pain that worsens with movement.
- Inflammation or swelling near the greater trochanter.
- Pain that travels down the leg, especially along the iliotibial band.
- Hip joint stiffness, restricted range of motion and inability to sleep without discomfort on the afflicted side.
Risk factors & Causes of Greater Trochanteric Pain Syndrome
Although some aspects of Greater Trochanter Pain Syndrome are unclear, research suggests probable causes:
- Overuse: Repetitive stresses on the greater trochanter region during activities such as running, cycling, jumping or other sports like basketball and cricket. These activities involve recurrent hip movements that strain the tissues associated with the Great trochanter i.e. Trochanteric Bursa and Tendons of Gluteus Medius and Minimus.
- Trauma: Experiencing a fall or a direct injury on the lateral side of the hip, such as slipping and falling on a hard surface leading to inflammation and initiation of GTPS.
- Excessive pressure: Lateral hip ache after sleeping on it, where prolonged pressure can trigger GTPS.
- Poor movement patterns: More recent research has revealed gait or walking patterns may induce GTPS symptoms and increase tendon irritation.
- Gender: Research suggests that females are at a 4 times higher risk of developing GTPS, potentially due to the anatomical differences in hip and knee angles (Q-angle) and lateral hip loading.
- Weight: Overweight or obese people are suggested to be at a higher risk of developing GTPS.
Early Phase Management
Early diagnosis and prompt treatment of GTPS is important where conservative treatment can commence once the stage of pathology is understood. Conservative treatment of GTPS encompasses rest & icing. During this period, modifying daily activities may be required.
Medications such as NSAIDs may be utilised to alleviate inflammation and pain. An individualised, structured rehabilitation approach can then be implemented going forward.
Rehabilitation and Injury Prevention
In recent research, Boyd et al (2020) have suggested a multifaceted approach for effective treatment of GTPS. After initial activity modification and pain alleviation, an isometric and isotonic exercise regimen to restore the original range of motion and basic strength capacity is recommended. The exercises target the Iliotibial band, hip flexors, and glutes to improve muscle flexibility and reduce tension. Gradually, the focus is shifted towards regaining strength qualities (maximal strength and endurance) with exercises to improve muscle balance and stability of the hip targeting the tensor fascia latae and the gluteus medius.
In instances where conservative treatment fail, corticosteroid injections into the affected area to resolve inflammation may be required. In very acute cases, surgery such as endoscopic release of the iliotibial band and bursectomy may improve function.
To Finish
Although GTPS affects many individuals where symptoms can be mild or acute, it is a treatable condition with early rehabilitation and management of the condition crucial to return to daily activities. To that end, it is important to individualise treatment to the symptoms you may be experiencing.
Combining education, treatment protocols including prescribed exercises enables individuals to take charge of their healing process to ensure the best outcome. Implementation of a personalised rehabilitation program combined with treatment of the underlying causes of GTPS, can aid in restoring hip and pelvic mobility, strength, and function.
If you are experiencing symptoms and are dealing with pain or discomfort in the hip region, consider a physiotherapy consultation for tailored guidance and treatment.
Book Now
References
- Collée, Gerard et al. “Greater trochanteric pain syndrome (trochanteric bursitis) in low back pain.” Scandinavian journal of rheumatology 20 4 (1991): 262-6 .
- Redmond, John Mark et al. “Greater Trochanteric Pain Syndrome.” Journal of the American Academy of Orthopaedic Surgeons 24 (2016): 231–240.
- Williams, Bryan S. and Steven P. Cohen. “Greater Trochanteric Pain Syndrome: A Review of Anatomy, Diagnosis and Treatment.” Anesthesia & Analgesia 108 (2009): 1662-1670.
- Klauser, Andrea S. et al. “Greater Trochanteric Pain Syndrome.” Seminars in Musculoskeletal Radiology 17 (2013): 043 - 048.
- Speers, Christopher Jb and Gurjit S Bhogal. “Greater trochanteric pain syndrome: a review of diagnosis and management in general practice.” The British journal of general practice : the journal of the Royal College of General Practitioners 67 663 (2017): 479-480 .
- Kong, Andrew et al. “MRI and US of gluteal tendinopathy in greater trochanteric pain syndrome.” European Radiology 17 (2007): 1772-1783.
- Baek, Dong Jin et al. “Greater trochanteric pain syndrome due to tumoral calcinosis in a patient with chronic kidney disease.” Pain physician 17 6 (2014): E775-82 .
- Thomassen, Peter Joachim Bruun et al. “Endoscopic Treatment of Greater Trochanteric Pain Syndrome - A Case Series of 11 Patients.” Journal of Orthopaedic Case Reports 9 (2019): 6 - 10.