The ankle is one of the most undervalued part of the body until you twist it - only then does one realize how vital it is to daily life and sport. Ankle sprains occur when the ankle is excessively rotated beyond its normal range of motion, causing the ligaments to stretch, tear or even rupture. completely. It is usually result of trauma i.e twisting during a fall or landing after a jump, or from uneven ground surfaces. Inadequate rehabilitation following these injuries can also result in chronic ankle instability and pain.
Ankle sprains are one of the most common injuries in the world, especially in athletes with research investigating the incidence of ankle sprains in Australia highlighting that these sprains account for 33 out of 43 ankle injuries in team sports. If you are a seasoned athlete or play sports for fun, the importance of ankle function can not be understated. In this piece, we dive deep into the ankle joint anatomy, mechanism of sprains and how we can effectively manage & prevent them, reducing their negative impact on our daily routines and function.
Anatomy of the Ankle
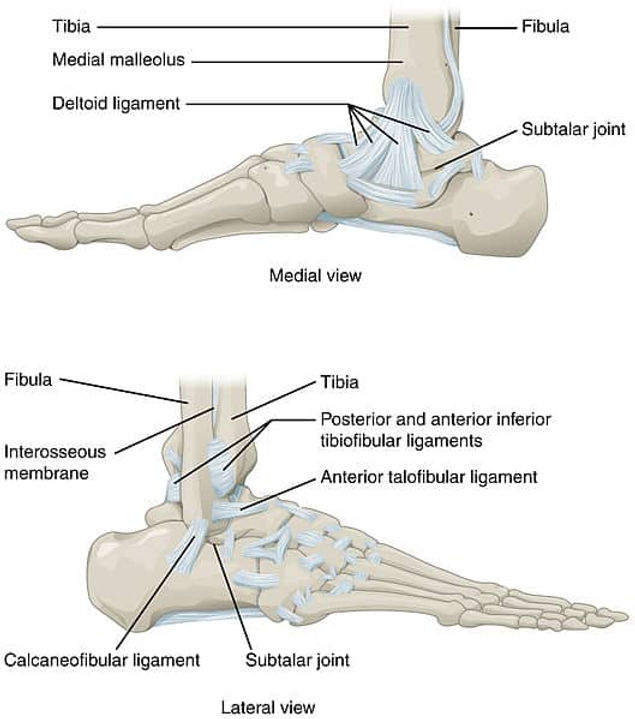
Before diving into the details of the Ankle sprain, it is essential that we understand the intricates of the structures that make up the ankle. The ankle joint is the union of lower leg and the foot and is compromised primarily of three bones: Tibia (shin bone), Fibula (outside leg bone) and the Talus. The intersection of these bones is called the Talocrural joint. The other key ankle joint, the sub-talar joint, is made up of the Talus and Calcaneus bones.
These two joints make perform two movements:
- Dorsiflexion & plantar flexion (talocrural)
- Inversion & eversion (subtalar)
Various muscles act on the ankle joint to provide these movements including the anterior shin muscles (such as Tibialis Anterior), posterior leg muscles (such as Gastrocnemius and Soleus), lateral leg muscles (such as Peroneals) and intrinsic foot muscles.e and acts to minimise joint friction. It is the degeneration of these cartilages which causes Osteoarthritis.
Key Ligaments - the Pain Points of Ankle Sprains
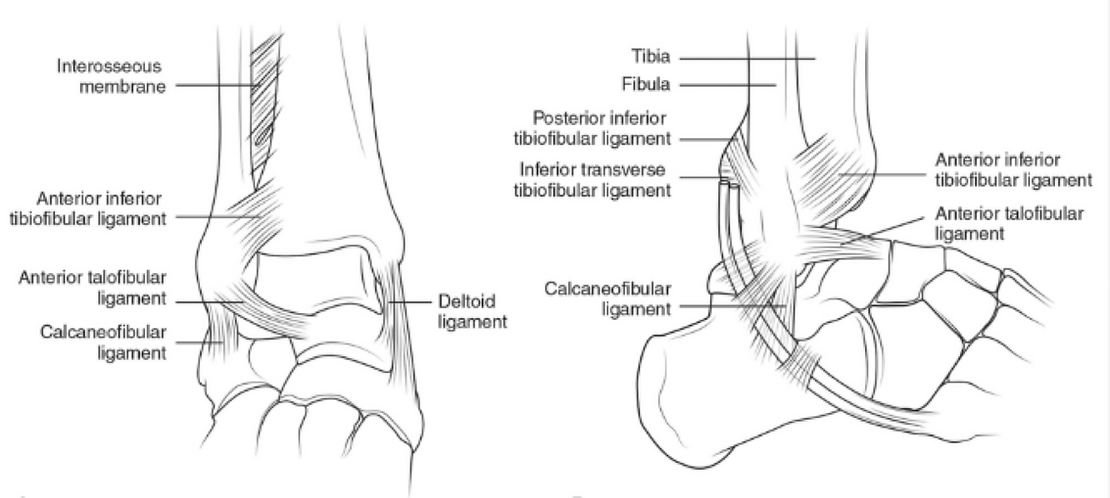
Ligaments act to connect bone points together and provide stability and support for the ankle and its joints. Two of the most commonly injured ligament groups injured are the lateral ankle complex and the syndesmosis:
- Lateral Ankle Complex: This complex is made up of three key ligaments - anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL) and posterior talofibular ligament (PTFL). These ligaments stabilise and minimise inversion movement (foot rolling in).
- Syndesmosis Complex: The syndesmosis is made up of anterior inferior tibiofibular ligament (AITFL) the posterior inferior tibiofibular ligament (PITFL) and the interosseous membrane. These ligaments stabilise and minimise excessive dorsiflexion and external rotation.
Assessing the Ankle - Differentiating Between Lateral Ankle & Syndesmosis Sprains
Clinically, it is differentiated from lateral ankle sprain by a lack of swelling, and tenderness at distal tibiofibular joint. A specific test for Syndesmosis performed by ‘squeezing’ fibula and tibia at midcalf region, if pain is elicited then Syndesmosis is confirmed. In contrast, the majority of ankle sprains are due to over-inversion (inward rolling of the ankle joint), with the ATFL most commonly injured. Clinically there is usually pain, bruising and swelling around the lateral ankle.
Clinical assessment includes an assessment of gait (walking mechanics), swelling measurement and pain on palpation. Patient is also asked if they have a prior history of ankle injury as they may be more prone to sprains. Clinical tests provide information about the stability of the joint and is useful for making decisions regarding the requirement for imaging or surgical opinions.
Rehabilitation & Therapy
Rehabilitation and therapy includes the following key aspects:
- Baseline Testing: Baseline testing provides a measure of key features important for ankle function and return to performance including ankle strength, range of motion and balance.
- Swelling & Pain Management: Strategies such as cryotherapy, taping and compression garments may be used to minimise swelling and regain range of motion.
- Exercise Prescription & Gait Re-Training: Exercises will be utilised to improve ankle range of motion and contractile qualities. Gait re-education is important for the early phases of rehabilitation to return the ankle to normal joint mechanics and loading patterns that allow for transition to running and other complex, high-load actions.
- Strength, Reactive Power & Proprioception: The latter stages of rehab include high loading strength and power training to recondition the joint ready for sport and activity. Proprioception and balance training are also a key theme, helping to reduce the risk of re-injury.
- Re-Testing & Return to Sport/Activity: Follow-up testing provides data-driven insights into ankle performance and if the joint is ready to return to sport/activity. A graduated return to performance plan is designed to ensure the ankle is ready to return to function.
Injury Prevention
Following tips prove beneficial in Injury prevention:
- Appropriate Footwear: Shoes that provide support to your feet are essential to maintain ankle stability, especially for athletes and injury prone individuals
- Warm-Ups: Directly starting your workout without warming the joint and surrounding tissue increases the risk of injury. This it is essential that you prepare your muscles and joint for workout that optimises strength and reactive qualities.
- Muscle & Joint Strengthening: Muscle strength is important for stability, especially during high loading tasks such as running and jump landings. Exercises that focus on surrounding muscles strength including calf muscles are essential to prevent further injury to the ankles.
To Finish
Although frequent, ankle sprains need to be thoroughly understood and managed to avoid long-term effects. A successful recovery depends critically on the complex anatomy of the ankle, differential diagnosis considerations, thorough evaluations and testing, and data-driven rehabilitation. Furthermore, the general health and endurance of the ankle joint is influenced by injury prevention strategies and continuous strength training to optimise ankle function.
Prevention outshines cure! If experiencing symptoms or have sustained an ankle injury, consider a physiotherapy consultation or musculoskeletal screening and testing consultation for tailored guidance.
Keep active and performing! 🏃♀️🏃♂️
Book Now
References
Fong, D.TP., Hong, Y., Chan, LK. et al. A Systematic Review on Ankle Injury and Ankle Sprain in Sports. Sports Med 37, 73–94 (2007)
Gray H. Arcturus Publishing; 2009. Gray's anatomy: with original illustrations by Henry Carter
Procter P., Paul J. Ankle joint biomechanics. J Biomech. 1982;15:627–634McCluskey LC, Black KP. Ankle injuries in sports. In: Gould JS, et al., eds. Operative
McCluskey LC, Black KP. Ankle injuries in sports. In: Gould JS, et al., eds. Operative foot surgery. Philadelphia: Saunders, 1994:901–36
Boytim MJ, Fischer DA, Neumann L. Syndesmotic ankle sprains. Am J Sports Med. 1991;19:294-8
van Dijk CN, Lim LS, Bossuyt PM, et al. Physical examination is sufficient for the diagnosis of sprained ankles. J Bone Joint Surg Br 1996;78:958–62
Knight KL. Initial care of acute injuries: the RICES technique. In: Cryotherapy in sport injury management. Champaign, Ill.: Human Kinetics, 1995:209–15
Disclaimer: This blog is for informational purposes and should not be considered a substitute for professional medical advice. Please consult with our qualified healthcare providers for personalised recommendations related to your specific condition and needs.