Ankle stiffness and pain in the morning upon wakening? Noticed a persistent ache develop after rigorous running? If so, you may be dealing with an Achilles tendinopathy, a common enemy for those who lead physically active lives. Research suggests that approximately 24% of athletes experience this injury in their careers with runners having an incidence of 9 injuries per 1000 hours of running.
If you are experiencing pain the the calf/heel region or suspect Achilles tendinopathy, then stick rill the end of this article and find out what this condition is, how it develops and how we can effectively manage it.
What is Achilles Tendinopathy? What are the Associated Risk Factors?
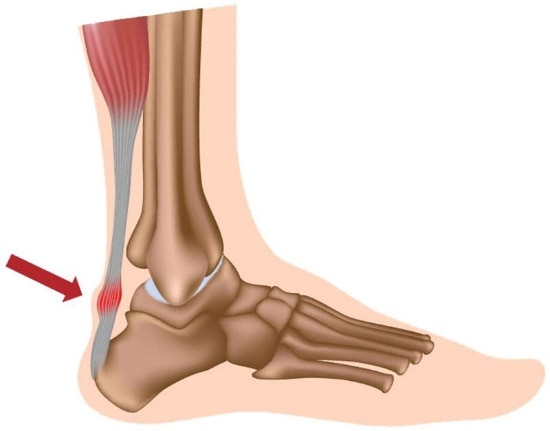
Before we discuss Achilles Tendinopathy, we must discuss the Achilles Tendon itself. The Triceps Surae is a term used to group the calf muscles - gastrocnemius, soleus and plantaris muscles. The Achilles tendon is the connection between these muscles and the back of the heel (calcaneus). Research has suggested what makes the Achilles tendon prone to injury is the less vascularized area in the 2 to 6 cm region near its union with the calcaneus bone.
Certain factors that predispose the Achilles tendon to injury are:
- Excessive Strain: Physically active individuals like Runners, Basketball and football players can overload the tendon, causing acute inflammation and long term changes to tendon structure.
- Mechanical Abnormalities: Deviation from normal foot structure i.e. anomalous foot cavity shape can lead to an increased risk of developing Achilles Tendinopathy.
- Sudden Spikes in Training Loads: A quick increase in training sessions, inadequate warm-up and cool-down regime and inappropriate form during exercise can result in overload and pain to the Achilles tendon.
- Muscular Deficiencies: Increased tightness in the calf muscles leads to decreased flexibility, potentially increasing the loading through to specific portions of the tendon.
- Body Weight: Excessive body weight or Obesity can exert excessive stress on the Achilles tendon predisposing it to injury.
The continuum model from Jill Cook’s research suggests that Tendinopathy develops in three phases: reactive tendinopathy, tendon dysrepair and then degenerative tendinopathy. This means that a susceptible tendon may not be able to withstand normal loading forces leading to reactive tendinopathy. It is not well known at which age tendons become susceptible to tendinopathy, as tendon’s structure matures during puberty indicating that Achilles tendinopathy can happen at any age.
Signs & Symptoms
Achilles Tendinopathy presents itself as a multitude of symptoms. Knowledge of these symptoms is a first step towards early recognition of Achilles Tendinopathy. The condition may manifest through a spectrum of indicators, including:
- Pain in the heel region: The most common and hallmark symptom of Achilles Tendinopathy is persistent aching in the back of heel aggravated especially when you wake up and during physical activity.
- Swelling and tenderness: Swelling is observed in the region of the Achilles Tendon soon after injury.
- Decreased range of motion: Achilles tendinopathy decreases ankle flexibility, which reduces the ability to push off their foot from the ground. The Achilles tendon is frequently more stiff and uncomfortable in the early morning or following extended periods of inactivity.
Are All Achilles Tendinopathy Injuries the Same?
Achilles tendinopathy is a broad term comprising: Tendinitis - which is acute inflammation and Tendinosis which is chronic inflammation. They differ in many ways:
- Tendinitis which involves acute inflammation consists of conservative treatment and has a better recovery rate.
- Tendinosis is a persistent condition caused by recurrent trauma or an injury that has not healed completely, which can lead to changes in the Achilles tendon structure.
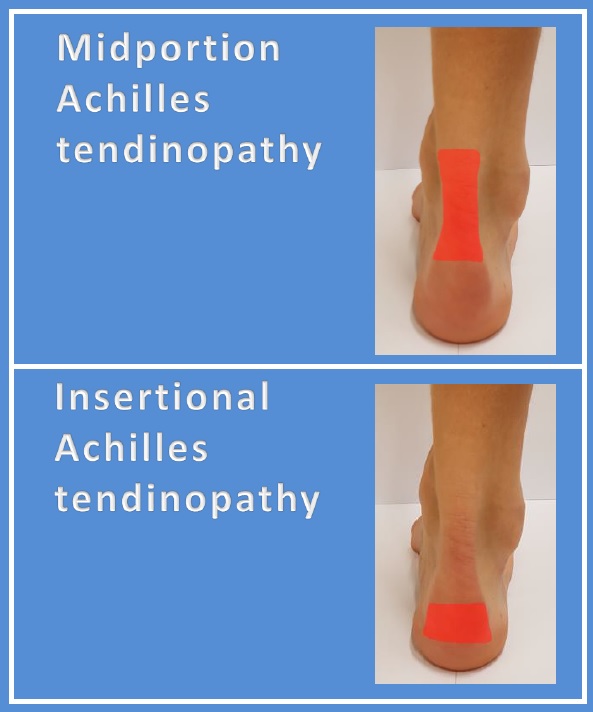
Achilles Tendinopathy is anatomically divided into two types according to the exact location involved:
- Insertional Achilles Tendinopathy: In this type, the affected area is the distal portion of the Achilles tendon, approximately 2cm, extending till its insertion point into the calcaneus bone.
- Mid-Portion Achilles Tendinopathy: This type of Achilles Tendinopathy occurs in the middle third of the Achilles Tendon approximately 2 to 6 cm proximal to the calcaneus bone.
It is important to distinguish the location of injury, as rehabilitation targeted towards mid-portion tendinopathy may in fact aggravate an insertional tendinopathy.
How is Achilles Tendinopathy Managed?
Conservative treatment is the first line of treatment for Achilles Tendinopathy. Understanding the tendon’s function and the stage of pathology is crucial to effective management. For an acute tendonitis (inflammation of the tendon), rest and anti-inflammatories can reduce pain along with a graduated rehab program.
That said, long standing chronic tendinosis requires a well designed loading and rehabilitation plan to enhance tendon health and function. Rest unfortunately fails to improve chronic tendinopathies, instead resulting in deconditioning to the tendon and surrounding muscles.
Wearing appropriate orthotic footwear can aid recovery by reducing pressure off the Achilles tendon hastening the recovery process.
Exercise Management
The type of exercises employed and how these exercises are performed are important for chronic tendinopathies. The two types of muscle contractions that are important in tendinopathy rehabilitation are: isometric and eccentric exercises
- Isometric Loading: Isometric exercises involve only muscular contractions sparing joint movements. These exercises allow joint strengthening without putting an undue amount of strain on it, reducing pain.
- Eccentric Loading: Eccentric exercises focus on the lengthening phase of muscular contraction focusing on muscle adaptability and may be gradually added into the rehabilitation regimen. Eccentric exercises include eccentric calf raises and seated soleus raises.
Progressive Loading - The Key to Long Term Adaptation
Managing re-loading the Achilles tendon during rehabilitation is important to avoid re-injury. For those returning to running, managing and controlling several variables allows for progressive reconditioning:
- Volume: Reducing total volume and assessing response to loading allows for progressive load increase. Methods such as the acute:chronic workload ratio along with symptom/wellness monitoring allows for specific tracking and increases in running volume.
- Intensity: Initially, the pace of your sessions may be slower to reduce tendon elastic loading.
- Frequency: Frequency may be reduced initially to allow for adaptation between running sessions, with this gradually increased as volume increases.
- Running Gait: Different running surfaces and conditions might affect how much strain is put on the Achilles tendon. Selecting the right shoes and adjusting to the terrain are essential factors.
- Cross-Training: By varying the physical demands placed on the body, low-impact exercises and cross-training methods reduce loading to the Achilles tendon and help to maintain cardiovascular health and fitness.
To Finish
Although Achilles tendinopathy affects a wide range of active individuals, it is a treatable condition with effective rehabilitation and management. Early management is crucial to reduce the risk of tendinitis developing into chronic tendinosis. Effective strength rehabilitation programming and load management are the key to Achilles tendinopathy management. A holistic approach is also important - to identify the causative factors to developing Achilles tendinopathy (biomechanics, loading, weakness) to ensure risk of re-injury is reduced and performance is optimised.
If you’re experiencing symptoms or have flair ups in Achilles pain, consider a physiotherapy consultation or musculoskeletal screening and testing consultation for tailored, data-driven guidance.
Book Now
References
Colbert LH, Hootman JM, Macera CA. Physical activity-related injuries in walkers and runners in the aerobics center longitudinal study. Clin J Sport Med. 2000 Oct;10(4):259-63.
O'Brien M. The anatomy of the Achilles tendon. Foot Ankle Clin. 2005 Jun;10(2):225-38.
Mahan J, Damodar D, Trapana E, Barnhill S, Nuno AU, Smyth NA, Aiyer A, Jose J. Achilles tendon complex: The anatomy of its insertional footprint on the calcaneus and clinical implications. J Orthop. 2020 Jan-Feb;17:221-227
Abate M, Salini V. Mid-portion Achilles tendinopathy in runners with metabolic disorders. Eur J Orthop Surg Traumatol. 2019 Apr;29(3):697-703.
Longo UG, Ronga M, Maffulli N. Achilles Tendinopathy. Sports Med Arthrosc Rev. 2018 Mar;26(1):16-30.
Maffulli N, Kenward MG, Testa V, Capasso G, Regine R, King JB. Clinical diagnosis of Achilles tendinopathy with tendinosis. Clin J Sport Med. 2003 Jan;13(1):11-5
Vo TP, Ho GWK, Andrea J. Achilles Tendinopathy, A Brief Review and Update of Current Literature. Curr Sports Med Rep. 2021 Sep 01;20(9):453-461
McClinton S, Luedke L, Clewley D. Nonsurgical Management of Midsubstance Achilles Tendinopathy. Clin Podiatr Med Surg. 2017 Apr;34(2):137-160
Disclaimer: This blog is for informational purposes and should not be considered a substitute for professional medical advice. Please consult with our qualified healthcare providers for personalised recommendations related to your specific condition and needs.